Informing Medicine Users About Side Effect Risk Peter Knapp
Poster Presentations
- Pain levels following Day Case Surgery. Impact of Pharmacist Counselling.
- What Contribution does a PODs Scheme make to Improving Medicine Mismanagement?
- Effectiveness of a Pharmacist-Led Outpatient Clinic For Symptomatic Relief of Irritable Bowel Syndrome
- Evaluation of a Continuing Professional Development project for hospital pharmacists
- To Glove or not to Glove...........that is the question
- South West Pharmacy Assistant Accredited Training Scheme
- Availability and Appropriateness of Medicines Information for the Paediatric Population
- Intravenous drug use in the Intensive Care Unit (ICU)
- Intervention Monitoring in the Dispensary
- The unlicensed use of oral ketamine - provision of information to General Practitioners and patients
- Inappropriate Secondary Care Prescribing of PPIs has a Significant Influence on Primary Care: Fact or fiction
- The use of a patient focus group to development a holiday travel information booklet for patients on lithium
- Re-engineering pharmaceutical care for Ear Nose and Throat (ENT) patients
Keynote Address
The President, Helen Remington, opened the Weekend School to the strains of "Also Sprach Zarathustra" ; the theme from "2001:A Space Odyssey".
In her address to the audience, she launched the joint GHP/RPSGB leaflet on Hospital Pharmacy, the GHP IT Special Interest Group and the GHP 5 year Strategy. She also announced the winners of the GHP Hospital Pharmacy Effectiveness Award, the result of the MSF/AEEU merger ballot and that the results of the AAH survey on the Weekend School would be the subject of a talk later on in the weekend. She stated that due to the late issuing of papers, there would be no Annual General Meeting at the School, but that it would be held on 13th June in Birmingham.
Dr Smith explained that he was a last minute replacement for Lord Hunt, Undersecretary of State for Health, who was unable to attend. He dealt with implementing the English NHS Pharmacy Programme, the current issues and progress to date. The whole process involved
- shaping and re-engineering services
- continuous improvement in quality
- making better use of the skills and dedication of staff
- ensuring pharmacists can use their skills to ensure patients get the best from their medicines
- getting structures right - designing services around patients
- making best use of pharmacists and support staff
He went on to talk about extended prescribing rights, local pharmaceutical services, the NSF for Older People, concordance and patient partnership, service quality and clinical governance. He completed his talk with a discussion on workforce and skill mix issues.
The NHS plan contains many messages for all of us in the National Health Service. However, the overriding theme is how we put the patient at the centre of all of our activities. It is as much about how we do things as what we do. This talk will give examples of how this has been implemented in practice in a hospital.
University Hospital Lewisham is located in South East London in an area of high socio-economic deprivation. It has 600 beds, 2,500 staff and an income of £100m. It is described as a DGH plus as, in addition to the usual range of hospital services, it has considerable undergraduate medical teaching and an R &D portfolio.
As a result of the NHS plan we are re-designing our models of care and patient processes around the needs of patients. A number of examples will be highlighted in the presentation.
Primary Care Centre, radically reducing waits in the A & E department, informing and empowering patients
Greater use of electronic technology leading to electronic patient record - enabling booking and scheduling of patient care and electronic communications with GPs
Cancer collaborative which has been based on the patient journey and the patient perspective of care
Improved out-patient services with 97% of patients being seen within NHS Plan standards, partial booking arrangements radically reducing DNAs
Reconfiguration of emergency and elective services to reduce and eliminate cancellations
Involvement of patients as citizens through PALS and Local Authority Scrutiny
|
'Future Visions'
Stephen Freeborn,
Director of Pharmacy. Salford Royal Hospitals NHS Trust. |
 |
Starship Pharmacy-The New Frontier, (Director's Log, Stardate 06.04.01)
I will start the talk with a brief overview of my life experience of Pharmacy and how Pharmacy roles have changed from the medicinal preparation days to the information science and treatment provider role that we will increasingly be involved in. I will then develop the argument for our involvement in the NHS Plan and ask the question 'Why bother?' At this point the huge agenda of Medicines Management will be introduced with reference also to Clinical Governance, NICE and CHI.
The next part of the talk will explore the Re- engineering of Pharmacy Services with particular reference but not solely to Hospital Pharmacy. This part discusses Electronic Prescribing, Robotics and e-Pharmacy. The final section will concentrate on Staff recruitment, retention, training and education with examples of innovative use of different grades of Pharmacy staff. The conclusion of the talk will emphasise our need to be fit for purpose, realistic and completely patient focussed.
|
Baxter IV Award lecture
Validation of Disinfection Techniques in Hospital Aseptic Dispensing Units
Hiom, S.J.
Pharmaceutical Unit, St.Mary's Hospital, Penarth, Wales, UK. |
 |
Summary
Current in-house methods of validating aseptic transfer are insensitive and are not appropriate methodologies for accurately assessing the disinfection process. The aims of this study were therefore to:
- develop an accurate disinfection assessment method
- use this to determine the optimum disinfection regimen
- compare this method with current in-house techniques
Four disinfection techniques were assessed:
- Spray 70% IMS + 2 min lockout
- Spray 70% IMS - no lockout
- Wipe with 70% IPA
- Spray 70% IMS + wipe with IPA
A total immersion method of enumeration was developed and was six times more sensitive at microbe detection when compared with the established roll plate method.
Statistical analysis of the results showed that wiping with IPA alone or with IMS spraying showed significant advantage over spraying alone and that spraying with IMS was as effective after 10 second exposure as 2 minutes.
This total immersion method may also be used for training and in-house validation of staff techniques.
The move towards evidence based medicine has been re-inforced by the National Plan for the NHS. The evidence relates to both the treatments we use and the way we deliver those treatments.
Pharmacy practice research in both the hospital and primary care sectors has to be a priority, as medicines are the most commonly used intervention and the way that pharmacy services are delivered is under-researched.
How we approach this task in the secondary care sector will be analysed using Kipling's six honest serving men of What and Why and When and How and Where and Who.
The search for the ultimate solution to our post-registration developmental needs is unlikely to have been completely successful. In order to find our "Holy Grail" we need a clear picture of that which seek. There are many different views as to what we are trying to achieve so knowing when we get there is difficult.
In this presentation I will describe the pathway that we have been following and the goals we have achieved so far. I will then describe the leap of faith we have taken to move on from the ubiquitous Diplomas to a structured career development programme, which meets the needs of the service as well as the individual.
The newly introduced D.Pharm offers us an opportunity to increase the knowledge and practice of our middle grade pharmacists, before they specialise and develop new knowledge through the integral research programme. More experienced staff are catered for by exemption from some parts of the course. The scheme is service driven and, we hope, will provide the consultant pharmacists of the future.
Workshops
Technicians: How do we unleash their potential?
Presenter: Barbara Wensworth
Course Tutor BTEC Applied Science - Pharmaceutical
The aim of the session is to explore how hospital pharmacists should develop and use the technician resource.
Objectives: At the end of this session participants will be able to:
- Identify current and future roles for technicians
- Identify barriers to the extension of technicians roles
- Develop strategies to overcome obstacles
- Present three key messages to the conference so that delegates can facilitate further service developments.
Pharmacists: The role in Primary Care
Presenter: Duncan Petty
Research Pharmacist, Division of Academic Pharmacy Practice, University of Leeds
The aim of this session is to give an overview of the roles of the pharmacist working in Primary Care and integration with Secondary Care pharmacy.
Objectives: At the end of this session participants will be able to:
- Describe the role of the Primary Care Organisation (PCO) and Practice pharmacist in medicines management
- Identify the opportunities for liaison across the interface.
- Present three key messages to the conference so that delegates can facilitate further service developments
Consultant Pharmacists: Meeting the challenge.
Presenter: Prof. Liz Kay
Chief Pharmacist, Leeds Teaching Hospitals NHS Trust
The aim of this session is to explore the strategies adopted by senior pharmacists in embracing the new NHS National Plan for pharmacy.
Objectives: At the end of this session participants will be able to:
- Identify potential roles of specialist pharmacists
- Describe the impact of the national plan in future pharmacy workforce requirements
- Present three key messages to the conference so that delegates can facilitate further service developments
Educating pharmacy for the NHS plan
Presenter: Rob Swallow
Assistant Director, Educational Development, University of Manchester
The aim of this session is to explore the continuing education requirements of the pharmacist workforce, and the challenges associated with the NHS plan, particularly relating to hospital practice.
Objectives: At the end of this session participants will be able to:
- Identify key changes in educational requirements to meet the needs of the NHS plan
- To identify appropriate methods of meeting identified requirements
- Present three key messages to the conference so that delegates can facilitate further professional developments
The Paediatric Clinical / Compounding Interface Group
Chairs: Val Wells1 and James Wallace2
1 Alder Hey, 2 Yorkhill, Glasgow
The aim of the session is to explore the issues affecting pharmaceutical use in paediatrics. To consider means of improving pharmaceutical availability in order to meet clinical requirements.
Objectives: At the end of this session participants will be able to:
- Understand the available alternatives for paediatric patients - including licensed use, "off label" use, alternative routes of administration, overseas licensed products, purchased "Specials" and extemporaneous preparation.
- Understand the risks and limitations of these alternatives.
- To rationalise the decision making process.
- To improve communication between the clinical and compounding pharmacists.
(Followed by a brief Compounding Interest Group AGM)
Christina Lowe Chair: The Paediatric Clinical / Compounding Interface Group.
Delivering the new NHS pre-registration training programme
Presenter: Julie Sowter
Pre-registration Pharmacists Programme Leader, Dept of Academic Pharmacy Practice, University of Leeds
The aim of this session is to explore the new pre-reg training programme with particular emphasis on secondary care.
Objectives: At the end of this session participants will be able to:
- Describe the key elements of the new pre-registration training programme.
- List changes required to integrate the pre-reg training programme into hospital practice
- Describe the local implementation of pre-reg competency assessment
- Present three key messages to the conference so that delegates can facilitate further service developments.
Unlicensed medicines: Managing the risk
Presenter: Liz Mellor
Lead Pharmacist for Clinical Governance, Leeds Teaching hospitals NHS Trust
The aim of this session is to give an understanding of the practical issues relating to the use of unlicensed medicines.
Objectives: At the end of this session participants will be able to:
- List the key implications of MCA Guidance Note 14
- Outline the legal issue of licensed vs. unlicensed medicines use
- Discuss the ethical issues associated with unlicensed medicine use specifically considering the issue of informed consent.
- Present three key messages to the conference
Dispensaries: A pharmacist free zone
Presenter: Andrew Barker
Chief Pharmacist, Doncaster NHS Trust
Aim Of The Session:
The aim of this session is to understand the value to patient care of removing pharmacists from dispensaries and to explore strategies that will facilitate the development of safe, efficient dispensaries without the need for a pharmacist's presence.
Objectives: At the end of this session participants will be able to:
- Identify the driving forces for the introduction of pharmacist free dispensaries
- Identify obstacles that may impair progress with pharmacist free dispensaries
- Develop strategies to overcome these obstacles
- Present three key messages to the conference so that delegates can facilitate further service developments
Procurement and Distribution Group: Supply chain management now and in the future
Chair: Allan Karr
Procurement and Distribution Interest Group
This session will deliver an update on future policies for procurement and distribution, appropriate training requirements and future use of technologies including robotics.
Debate
|
Pharmacists as independent prescribers
Chair: Helen Remington
For: Duncan McRobbie
Clinical Pharmacy Manager, Guys and St Thomas's Hospital, London
Against: Richard Cattell
Clinical Pharmacy Manager, United Bristol Hospitals NHS Trust
|  |
This debate will explore the advantages and disadvantages of the pharmacist as an independent prescribers.
"This house believes that all hospital pharmacists should be independent prescribers"
Seminars
The aim of this seminar is to update attendees on the contents of the NSF and provide focus on implementation.
Objectives: At the end of this session participants will be able to:
- List the key points of the framework
- Identify potential roles for pharmacy practice
- Develop strategies for local delivery
- Present three key messages to the conference so that delegates can facilitate further service developments
Therapeutics update: evidence based psychiatry
Chair: Peter Pratt
Chief Pharmacist, Community Health Sheffield NHS Trust
The aim on this session to provide a therapeutics update on evidence based psychiatry
Objectives: At the end of this session participants will be able to:
- The management of depression
- The management of schizophrenia
- The secondary prevention of dementia
Therapeutics update: Evidence based Cardiology
Chair: Sue Thomis
Cardiology Pharmacist, Bradford NHS Trust
The aim on this session to provide a therapeutics update in evidence based cardiology
Objectives: At the end of this session participants will be able to:
- Evidence based management of heart failure
- Evidence based management of acute coronary syndromes
- Evidence based management secondary prevention of myocardial infarction
Oral presentations
|
Yorkshire Clinical Pharmacy Audit
Acomb C 1 , Alldred A C 2 , Taylor P 3 , Proctor J 4
Departments of Pharmacy: Bradford Royal Infirmary1, Leeds Teaching Hospitals2, Airedale General Hospital3, Scarborough General Hospital4 |

Chris Acomb |
Introduction
The Yorkshire Region senior pharmacy managers set up a number of audit projects in the 1990's e.g procurement and aseptic services. Following their success they formed a small working party to develop an audit of clinical pharmacy services in 1997. This paper describes the development of a clinical pharmacy audit group and the development of standards and audits.
Objectives
To identify the current breadth of clinical pharmacy services within the Yorkshire region.
To identify methods for developing and improving clinical pharmacy services within an agreed framework.
To develop a regional group of lead clinical pharmacists to move clinical pharmacy services forward.
Method
A small working group reviewed The Scottish Office document, Clinical Pharmacy in the Hospital Pharmaceutical Service: Framework for Practice1, to decide whether this matched practice in Yorkshire. From this document a tool for the qualitative audit of clinical pharmacy services (QAS) was developed. This analysed the range of services provided by Trusts and whether policies and procedures supported them.
Following the development of the audit tool, a meeting was held to bring together a representative from each Trust within the Region. The audit document was discussed, clarified, agreed and implemented in September 1997.
The findings were reported in November 1997. This led to the formation of the Yorkshire Clinical Pharmacy Audit Group (YCPAG) comprising a representative from each Trust who identified strengths and weaknesses from the audit. YCPAG selected common problem areas to be the focus for the region's attention. Specific audit tools for these priority areas were developed. The first specific audit was the documentation of Pharmaceutical Care Plans (PCP's).
A structured approach to each specific audit was undertaken. The audit tool comprised; Structure, Process and Outcome components. A baseline audit was always undertaken. Following the baseline audit working groups were convened to develop good models of practice, training packages and policy. These structural components were shared and implemented. Following these interventions, a follow-up specific audit was then undertaken after approximately 12 months.
Results
Thirteen Trusts responded to the initial QAS. Some areas of practice were shown to be delivered consistently across the region. These included formulary management, patient counselling, pharmacist involvement in ethics committees and, education and training. However only a small percentage of Trusts had robust procedures for documenting Pharmaceutical Care Plans (23%) and Discharge Planning (30%). No Trust had a procedure for Drug History Taking.
Seven Trusts provided data for the specific audit of documenting PCP's. The results of the baseline and follow up audit are shown in Table 1. Following the intervention described, there was a significant increase in the number of pharmacists who had received training in pharmaceutical care planning. There was also a statistically significant increase in the main outcome component - the number of patients with a documented PCP. The number of patients screened for pharmaceutical care issues also increased although this was not statistically significant.
Table 1: Results of the specific audit: Documenting Pharmaceutical Care Plans (PCP)
| |
% of patients with
documented screening |
% of patients with
a documented PCP |
% of Pharmacists
trained in PCP's |
| Trust |
Baseline
May 1998 |
Follow up
Dec. 1999 |
Baseline
May 1998 |
Follow up
Dec. 1999 |
Baseline
May 1998 |
Follow up
Dec. 1999 |
| 1 |
90 |
100 |
100 |
89 |
0 |
36 |
| 2 |
100 |
100 |
0 |
50 |
0 |
100 |
| 3 |
0 |
86 |
0 |
62 |
0 |
100 |
| 4 |
0 |
97 |
0 |
100 |
0 |
100 |
| 5 |
50 |
37 |
0 |
51 |
0 |
35 |
| 6 |
100 |
100 |
89 |
95 |
62 |
62 |
| 7 |
0 |
83 |
0 |
83 |
0 |
100 |
Mean
(SD) |
48.6 (48.5) |
86.1 (22.8) |
28.3 (48.7) |
75.7 (21.0) |
8.9 (23.4) |
76.1 (31.0) |
| t test |
|
0.09 |
|
0.02 |
|
0.01 |
Discussion
Prior to 1997, there was widespread disparity in clinical practice across the Yorkshire region. This made it difficult to audit specific areas of clinical activity. The formation of the regional group resulting in collaboration, facilitated a common approach to practice and the development of regional standards. Pharmaceutical care planning was selected as the first audit as a small number of Trusts had outline polices which they were willing to share. Care planning is an integral component of practice from which the majority of patient focused care hinges. The group felt it was essential to raise the standard of pharmaceutical care planning as a priority. This specific audit demonstrates significant improvement in the standard of practice in a large number of Trusts in documenting PCP's.
Building on the success and enthusiasm of the regional group we have developed further audits in discharge planning. In addition the audit has identified new training needs and areas for practice research.
References
1. The Scottish Office document, Clinical Pharmacy in the Hospital Pharmaceutical Service: Framework for Practice
Introduction
A First Class Service1 proposed a culture of lifelong learning in which Continuing Professional Development programmes are used to identify and meet the learning needs of individual health professionals. It defines CPD as 'a process of lifelong learning for all individuals and teams which meets the needs of patients, delivers the health outcomes and healthcare priorities of the NHS, and which enables professionals to expand and fulfil their potential.'
A later Health Circular, 'Continuing Professional Development: Quality in the new NHS' added that 'CPD should be a partnership between the individual and the organisation; its focus should be the delivery of high quality NHS services as well as meeting individual career aspirations and learning needs' and stated 'By April 2000 the majority of health professional staff should have a personal development plan (PDP)'2.
Subsequent to this, informal discussions with senior staff in July 1999 showed that there were considerable misunderstandings around CPD and very little progress had been made on introducing CPD. There was concern about how to achieve NHS deadlines and anecdotal cries for help.
Currently within pharmacy there is no co-ordinated approach to CPD. Organisations such as the College of Pharmacy Practice provide a structured framework for professional development for pharmacists, however we needed to look more widely at NHS needs and cater for all the staff involved in providing a pharmacy service.
Method
Once the need was established we consulted widely to develop a strategy to support pharmacy staff. We set up a working group (jointly between the then North Thames and South Thames regions) which represented a cross section of our service users. This group met initially in November 1999 and developed the following strategic objectives and proposals
Strategic objectives
To increase understanding and awareness of CPD amongst pharmacy staff
To facilitate a culture of life long learning and reflective practice
To encourage pharmacy staff to compile and maintain their own portfolio of CPD activity
Recommendations
- Promote CPD to senior pharmacy managers
- Identify a lead person (facilitator) in each hospital and health authority to promote CPD within their workplace, and provide support to their colleagues
- Provide guidance on ways in which CPD can be implemented within the workplace
- Provide training and support for the local facilitators
- Develop a training pack and marketing materials for use by the facilitators to train and motivate pharmacy staff
- Pursue funding for new regional posts to support the facilitators to implement CPD
The working group felt strongly that facilitation was a key factor in enabling the culture change required to move to reflective practice.
Results
Initial support activities
- 107 pharmacists and technicians from 62 of 69 hospital trusts and 11 of 26 health authorities from both regions attended a two-day facilitator training course by June 2000
- Developed a CPD training support pack for facilitators to use to help staff understand the main principles of CPD
- Working group developed guidance for implementation within departments
- Logo and promotional materials designed and produced
- Portfolio suitable for use by all grades of staff developed
- Successful bid to E&T consortia for additional funding, and recruitment of a team of part-time CPD regional co-ordinators in August 2000 for 1 year. These pharmacists visit organisations and support the local facilitators
Challenges
- Dispelling misapprehension about what CPD really is and how it differs from continuing education
- Variable support from senior pharmacy managers for their local facilitators
- Motivating and maintaining the enthusiasm and momentum of facilitators who have considerable time pressures and do this role on top of the 'day' job
- Lack of perceived deadlines by the local facilitators
- Development the facilitation skills and confidence of facilitators to proactively facilitate reflective practice
- Helping facilitators to encourage reflection and reflective practice in individuals
- Lack of competences for individuals to assess themselves against in developing their personal development plan
Ongoing support activities
Ongoing support for the facilitators was identified as a key area of activity, resulting in
- A team of CPD regional co-ordinators to visit facilitators to encourage, motivate, help problem solve, share good practice
- Ongoing CPD facilitator training - another 40 facilitators trained since September 2000.
- Regular CPD facilitator meetings to give opportunity to network, share experiences and meet ongoing development needs
- A focus on developing facilitation skills and confidence of facilitators in CPD facilitator meetings and during CPD regional co-ordinator visits
- Recent development of reflective practice support pack in response to needs identified by facilitators
- CPD regional co-ordinators soon to start onsite training of facilitators in several trusts where larger numbers of facilitators are required to effectively pump prime CPD
Future
The CPD working group (now to meet on a uniregional basis) continues to consider
- the ongoing support needs of pharmacy staff in the region
- a full evaluation of the strategy over the next couple of months looking at
- attitudes and commitment of individuals
- uptake and recording of CPD within departments
- value of CPD regional co-ordinators
- what bids to the education & training consortia are required to fund this support
References
1. NHS Executive. A First Class Service: Quality in the new NHS (HSC1998/113). London: HMSO; 1998. http://www.open.gov.uk/doh/coinh.htm
2. NHS Executive. Continuing Professional Development: Quality in the new NHS (HSC 1999/154). London: HMSO; 1998. http://www.open.gov.uk/doh/coinh.htm
Introduction
The planned new Code of Ethics says.."pharmacy managers have a responsibility to ensure that pharmacists have the requisite knowledge, skill and fitness to perform work delegated to them and also to comply with work instructions....." 1 The current checking accreditation for pre-registration students is 1.2.12 in the practical unit of the preregistration manual, relating to dispensing2. We introduced a requirement for newly qualified pharmacists to have a nominal 200 items double-checked using the same criteria as that in place for technical staff.
Assessing competence differs from performance appraisal. Competency assessment determines if an individual has the ability to perform the role. Performance appraisal assesses how well the individual performs the role. Registration as a pharmacist does not equate with competence to perform all the various clinical roles required of a pharmacist now or in the future. Developing both pharmacists' and technicians' clinical roles at ward level requires training, subsequent confirmation of competence and suitable methods for competence assessment. Provision of objective measures of the quality of the service is a key part of clinical governance. This work investigated current accreditation practices in the UK.
Objectives
- To establish if accreditation is in place for pharmacists.
- To establish which clinical activities are accredited.
- To establish methods of accreditation used.
- To obtain examples of methods, documentation and records of accreditation.
- To invite respondents to join a practice interest group.
Method
A questionnaire was designed and agreed by the education and training pharmacist, clinical services manager and chief pharmacist. After piloting, this was sent to all chief pharmacists of NHS hospitals and trusts listed in the Chemist and Druggist Directory 20013. A stamped addressed envelope was included and response within two months requested. Questionnaire results were entered onto a spreadsheet for analysis.
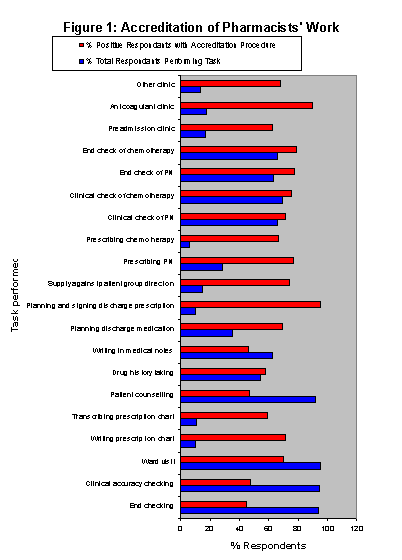
Results
Of 505 questionnaires distributed, 212 (42%) were returned and 206 (41%) completed. Of these 33% responses came from teaching hospitals, 21% of respondents were willing to share accreditation procedures and 39% were interested in joining a practice interest group. Initial results of the survey are shown in Figure 1. Some tasks in high-risk areas (e.g. clinical- and end-checking of chemotherapy and PN) were widely accredited (> 80%). High volume activities (e.g.clinical- and end-checking of dispensing, patient counselling) were only accredited in about 50% cases. Ward visits were widely accredited, possibly as a required practice activity for post-graduate qualification. Activities such as pharmacist-led clinics, prescribing chemotherapy, supply against a patient group direction and planning and signing for discharge medication, which were low volume (carried out by less than 20% respondents), but high risk tended to be highly accredited, in one case by as many as 95% of respondents. The most frequently reported accreditation methods were a) following a period of induction b) observation and c) competence-based assessment. Accreditation through evidence of continuing professional development was rarely reported, despite the requirements of clinical governance.
Discussion
Practical assessment of pharmacists and technicians has been described by authors in the US. Assessment methods for pharmacists and technicians included practical demonstration, written examination and open-book self-assessment4,5. Performance appraisal for clinical pharmacists is recommended in the Scottish clinical pharmacy practice framework6. This investigation has highlighted the wide scope of work remaining to be done in this field in the UK. The development of national accreditation with local flexibility is desirable for both pharmacists and technicians. The next step will be to set up a practice interest group to establish best practice from existing accreditation schemes and to work together towards developing national standards, both for tasks currently executed and for those under development.
References
1. Code of Ethics (Revised) Pharm J 2001;266:325-332
2. RPSGB Preregistration Training Manual 2000-2001.
3. Chemist and Druggist Directory 2001. 133rd Ed. United Business Media Ltd
4. Marshall JM et al. Practical, ongoing competency assessment program for hospital pharmacists and technicians. Am J Health-Syst Pharm 1997;54:1413-1417.
5. Martin AE, Stumpf JL, Ryan ML. 'Assessing pharmacists' competence in clinical information retrieval. Am J Health Syst Pharm 1996; 53: 2957-2958.
6. Scottish Clinical Pharmacy in the Hospital Pharmaceutical Service: A Framework for Practice 1996.
Introduction
Every medicine now supplied in the UK should be accompanied by a comprehensive patient information leaflet, written by the manufacturer, as required by European Directive 92/27 [1]. The Directive requires that all side effects listed in the medicine's Summary of Products Characteristics (previously known as the Data Sheet) should be included, in a form understandable to the patient. Empirical studies provide clear support for the view that patients do want to be given information about medication side effects [e.g. 2]
Most current patient information leaflets simply list all known side effects of the medicine, and rarely provide information on side effect frequency. An EU guideline [3] on side effect information, published after the Directive, recommends that the frequency of side effects should be described using one of five verbal descriptors varying from 'very common' to 'very rare' (see Table 1).
Table 1. Recommended verbal descriptors and EU 'assigned frequencies'.
| Verbal descriptor |
EU assigned frequency |
 |
Very common
Common
Uncommon
Rare
Very rare |
> 10%
1 - 10%
0.1 - 1%
0.01 - 0.1%
< 0.01% |
However, there does not appear to be any existing evidence showing that people's interpretation of these descriptors corresponds to the assigned frequencies. We therefore undertook two studies to test such interpretations.
Objectives
To measure people's estimates of side effect risk when given verbal or numerical information about hypothetical medicines.
Method
1) A convenience sample of 112 adults were given a hypothetical but realistic scenario relating to a fictitious antibiotic ('Epidoxin') given for a throat infection, which was reported to be associated with four side effects.
In a factorial design, they received either a verbal description of risk (the side effects are very common in people who take the medication) or a numerical description (the side effects occur in 15% of people who take the medication).
They were asked to estimate the probability that they would experience the side effects and to rate (on a Likert scale scored from 1 to 6) the impact on their compliance, risk to health and severity of side effects.
2) A convenience sample of 360 adults were given a hypothetical but realistic scenario relating to a fictitious antibiotic ('Epidoxin') given for a throat infection, which was reported to be associated with four side effects.
In a factorial design, they received one of four pieces of information: either a verbal description of risk about common side effects, rare side effects, or the numerical equivalent information (3% or 0.03%).
As before, they were asked to estimate the probability that they would experience the side effects and to rate (on a Likert scale scored from 1 to 6) the impact on their compliance, risk to health and severity of side effects.
Results
1) The mean probability rating of having the side effect was 64% (95% Confidence Intervals 59-70), if given the verbal descriptor 'very common'. Those given the value '15%' rated the probability at 20% (95% CIs 17-23). Those given the verbal descriptor also perceived side effects as more severe (mean difference 0.8, thought they would be more likely to suffer the side effect (mean difference 1.8) and would be less likely to take the medicine (mean difference 1.2), compared with those given the statistical information.
2) Those given the term 'common' rated the risk at 50% and those given '3%' rated the risk as 9.5%. Those given the term 'rare' rated the risk at 21%, as against 7% for those given '.03%'. As before, those given a verbal descriptor rated the severity of the side effects higher, the likelihood of occurrence higher and the risk to health higher. There was a greater impact of a verbal descriptor on their compliance for the 'common' category than for the 'rare' category.
Discussion
These studies conducted in samples of the general population suggests strongly that the verbal descriptions of side effect risk suggested by the EC Guideline lead to a gross over-estimate of risk. The studies showed a similar level of over-estimation of that risk. It became clear during these studies that the level of risk for individual side effects is often imprecise - the clinical trials are rarely large enough to calculate incidence rates with any certainty. This suggests that verbal descriptors may be an appropriate way to convey this information (reflecting the lack of certainty). What is needed, however, is a set of verbal descriptors that corresponds to relevant risk bands.
People cannot be expected to make informed decisions about medicine taking if they have a very a poor understanding of the risk of side effects occurring. It is surprising that respondents given the actual percentage risk consistently estimated a figure higher than that given and this warrants further research. Clearly, the studies reported here need repeating with representative patient samples, investigating the side effect risk of medicines actually being taken. Further research is also needed into alternative ways of presenting risk information to patients. However, in the mean time, authors of written information for patients about medicines should not use the terms recommended by the EU guideline.
References
1. Council Directive 92/27/EEC (OJ No L 113 of 30.4.1992, p.8)
2. Berry, D.C., Michas, I.C., Gillie, T. & Forster, M. (1997). What do patients want to know about their medicines and what do doctors want to tell them? A comparative study. Psychology and Health, 12: 467-80.
3. A guideline on the readability of the label and package leaflet of medicinal products for human use. EC Pharmaceutical Committee, 1998.
Posters
Pain levels following Day Case Surgery. Impact of Pharmacist Counselling
Conroy C. Cattell R. Waage K.
Department of Pharmacy. Bristol Royal Infirmary. United Bristol Healthcare Trust
Introduction
Over the past 2 years the annual number of day case surgery (DCS) operations within the Bristol Royal Infirmary (BRI) has increased by 27.3%. Patient preference and cost-effectiveness are among the principle reasons for this escalation (personal correspondence, DSU staff). Limitations do however exist. Successful day surgery requires effective management of pain in order to avoid delayed discharge and prevent re-admissions. Treatment of pain is therefore central to the care of the post-operative patient, the primary goal being the provision of effective analgesia with minimal/no adverse effects. A recent DCS audit of patient perception however highlighted a significant problem with post-operative pain, within the first two days of discharge. In June 1999, an Adult DCS Post-operative Analgesia Protocol was drawn up between the Clinical Pharmacy Manager and the DCS Surgeons. The protocol defined the conditions under which an appropriately qualified pharmacist could provide standard post-operative discharge analgesia and counselling to patients on discharge.
Objective
A pilot study was undertaken to determine whether implementation of a DCS Post-operative Analgesia Protocol improved pain control in patients in a Day Surgery Unit.
Method
Data was collected from consecutive day surgery patients over a four week period (control group - 2 weeks; study group - 2 weeks). Patients were considered eligible for inclusion if they (i) had undergone a DCS operative procedure (ii) were over 18 years (iii) had no contra-indications to the range of discharge analgesia available (co-codamol 30/500mg tablets, diclofenac 50mg tablets, diclofenac 100mg suppositories, co-dydramol 10/500mg tablets, paracetamol 500mg, ibuprofen 400mg).
During the first two weeks of the study, patients were supplied with their discharge analgesia following surgery and counselled by a member of the DSU nursing team (control group). The pain level of the patient was assessed using a visual analogue scale (VAS). Patients were asked to indicate by a single mark on a line numbered 0 to 10 their existing level of pain, where 0 represented no pain, and 10 represented the worst pain imaginable. Two days following their operation, patients were again asked to complete the VAS. The difference between the two scores was used to give an indication of how effective their post-operative analgesia was in reducing pain levels. Patients were also requested to give details of any additional analgesia they had taken over the two days, apart from that which they received on discharge.
Following baseline data collection, patients were recruited into the study group. Once a patient was considered medically fit for discharge from the DSU, the Pharmacist was bleeped to attend the discharge. The pharmacist was responsible for the dispensing, documentation and counselling of the patient regarding their discharge analgesia. In addition, patients received a patient information leaflet (PIL) regarding their pain relief, and were given the opportunity to clarify any aspects of their medication. At discharge, and two days following their operation the patient completed the VAS. Patients were again requested to give details of any additional analgesia they had taken over the two days, apart from that which they received from the pharmacist on discharge.
Results
Forty-three patients (23 males, 20 females) were recruited into the control group, and twenty patients (9 males, 11 females) were recruited into the study group. No patient supplemented their discharge medication with over the counter (OTC) analgesics. The data was classified according to procedure type. The difference in VAS score results for the control and study groups are presented in Table 1.
Table 1 Difference in VAS Score recorded following surgery, and two days after discharge in control and study group patients
| |
Control |
Study |
Procedure |
Number of
patients |
Difference in
VAS score
|
Number of
patients |
Difference in
VAS score |
| Lump Removal |
10 |
+1.20 |
9 |
+1.06 |
| Ganglion Removal |
4 |
+1.50 |
2 |
-1.00 |
| Dental Extraction |
5 |
+1.50 |
3 |
-0.66 |
| Arthroscopy |
14 |
0.00 |
3 |
-3.33 |
| Hernia Repair |
10 |
+1.80 |
3 |
-2.00 |
Data was normally distributed when the difference in pain level was plotted for all patients. A two sample t-test was performed using MiniTab(, and a statistically significant difference between control and study group patients was obtained (Mean (± SD) -0.93(1.65) versus 0.53(2.55), respectively, p=0.0085). This significance was maintained when Regression Analysis was performed for the variables sex (p=0.029) and operation type (p=0.002).
Discussion
Patient counselling has become a priority within the pharmacy profession since the relocation of focus from product to patient. Implementation of a DCS Post-operative Analgesia Protocol significantly reduced pain levels in patients. Providing more information, both verbal and written hence has important benefits. The results of this study are consistent with earlier research, demonstrating that patient care can positively benefit from the counselling given by clinical pharmacists1,2. As a consequence of this pilot work, it is evident that the role of the pharmacist in improving pain management through prescribing of analgesia within a 'group protocol', needs to be explored. Concurrent with the suggestions made in the NHS plan3, a study proposal for the latter has undergone Ethics approval, and will commence in July 2001.
References
1. Wandless I, Whitmore J. The effect of counselling by a pharmacist on drug compliance in elderly patients. Journal of Clinical Hospital Pharmacy. 1981; 6: 51-56.
2. Williford SL, Johnson DF. Impact of pharmacist counselling on medication knowledge and compliance. Military Medicine. 1995; 160: 561-564.
3. Pharmacy in the Future - Implementing the NHS Plan. Department of Health 2000.
What Contribution does a PODs Scheme make to Improving Medicine Mismanagement?
Nicholls M, Horler K, Conroy C, Cattell R, Campbell C.
Department of Pharmacy. Bristol Royal Infirmary. United Bristol Healthcare Trust
Introduction
As part of providing a service designed around the patient, the NHS encourages the uptake of patient own drugs (PODs) schemes1. Initiation of a study involving the reuse of PODs at the Bristol Royal Infirmary (BRI) resulted in considerable savings to both the Trust and the local Health Authority2. The PODs system has now been successfully implemented in surgical and medical wards at the BRI, following the appointment of two PODs technicians last year. Apart from the cost-savings attributed to less drug wastage with the PODs scheme, the system has highlighted a number of prescribing discrepancies, which may not otherwise have been detected during patient admission.
Previous published studies demonstrate that there is major room for improvement in constructing a patient drug history3,4. Discrepancies that occur during drug history taking are often transcribed from patient notes onto drug charts by junior doctors and can hence lead to medication administration errors (MAEs). In addition to co-ordinating the reuse of patient medication for discharge, PODs technicians at the BRI actively verify whether the drug history attained on patient admission by a junior doctor, is consistent with the details recorded on the chart. This ensures that any ambiguous information, which could be eventually misinterpreted by nursing or pharmacy staff, is clarified.
Objective
The objective of this study was to estimate both the number and type of drug discrepancies on patient admission, and hence quantify the effect of POD technician interventions on reducing medicine mismanagement.
Method
Within each Directorate, technicians assessed the suitability of PODs for reuse on a daily basis, and documented the individual drug history on a PODs Evaluation Sheet (PES). PODs technicians then interviewed each patient to determine whether they were taking any medication, other than that brought in on admission. The completed PES was then attached to the drug chart, and the information written on the drug chart and PES compared. Details of the type of error were recorded using a data collection form (DCF). Four headings relating to the type of error were used, including: incorrect strength/no strength; incorrect frequency/no frequency; omission of medication on chart (excluding medication which was deliberately omitted); other reason. In addition, details of the ward, date the error was spotted, and staff notified, was recorded. Once errors were identified, the PODs technician alerted medical or nursing staff, or attached a post-it sticker detailing the error, to the drug chart. This system ensured that any discrepancies were highlighted and resolved. Completed DCFs were then used to quantify the number and type of drug errors over a 3-month period.
Results
Over the first quarter of the PODs scheme, 219 medical and 109 surgical patients had their medication assessed by technicians on hospital admission. Following drug history taking, transcription of medicines by junior doctors onto charts was found to be incomplete in a number of instances, when compared with the information obtained by the PODs technician on the PES. The frequency and type of errors detected for each Directorate are presented in Table 1. Over a 3-month period, 1405 medicines were assessed, and 86 drug errors recorded. This represents a total of 6.1% of all items. In the main, doctors were informed about any discrepancies (70%). When not available, the Staff Nurse (23%) or Ward Pharmacist (7%) was made aware of any chart errors.
Table 1Errors detected on drug charts by PODs technicians on 11 medical and 6 surgical wards over a 3 month period
| |
Type of Error |
| Directorate
| Incorrect strength
/ no strength |
Incorrect frequency
/ no frequency |
Omission of medication on chart |
Other* |
| Medical (n=993) |
13 |
1 |
21 |
8 |
| Surgical (n=412) |
11 |
11 |
15 |
6 |
Total (n=1405)
Percentage of total |
24
1.7% |
12
0.85% |
36
2.6% |
14
1.0% |
n=number of PODs documented on admission (excludes discontinued items)
*Other reasons relate to omission of product brand, interactions, product withdrawal, or incorrect drug. In one case, the patient chart was endorsed with a drug that was entirely different from that documented on the PODs checklist on admission.
Discussion
This study demonstrates that 1 in every 16 medicines prescribed on admission are unintentionally different from previous medicines taken. This represents a considerable burden for the patient. The management of medicine at all stages of patient care has become a major priority in the new NHS plan1. Introduction of a PODs scheme not only delivers financial benefits2, but also contributes to reducing risk patients are exposed to by medicines. This further endorses the central role of the profession in medicines management.
References
1. Pharmacy in the Future - Implementing the NHS Plan. Department of Health 2000.
2. Campbell D, Cattell R, Conroy C. Waste not, want not. Health Service Journal 2000; 110: 31.
3. Taylor, S and Hughes, D. Emergency admissions (abstract). Pharmaceutical Journal. 1997; 259: 26.
4. Drewett, NM. Stop regular medicine error. Pharmacy in Practice. 1998; 8: 193-196.
Effectiveness of a Pharmacist-Led Outpatient Clinic For Symptomatic Relief of Irritable Bowel Syndrome
Parsons RWJ
Pharmacy Department, Kettering General Hospital
Introduction
Irritable Bowel Syndrome (IBS) is the commonest functional gastrointestinal disorder seen in both primary and secondary care and accounts for 20-50% of gastroenterology referrals in the UK1. IBS is a chronic recurrent disorder characterised by periods of exacerbation and remission. There is no clear clinical endpoint for it's treatment and management is often symptomatic and unsatisfactory1. IBS is traditionally diagnosed by Gastroenterologists and patients then referred back to their GPs for management and therefore places a huge burden on NHS resources, particularly valuable Consultant time.
The Pharmacist-led IBS clinic was established with patients referred for symptomatic management after recent diagnosis by a Consultant Gastroenterologist. The pharmacist was given prescribing privileges according to an agreed formulary. Patients were given thirty minute initial appointments and fifteen minutes follow-up appointments where all aspects of IBS were discussed and treatment initiated accordingly. Longer appointment times were used to aid the known high placebo response in IBS2 with more time spent with the patient to improve outcomes. A high quality Pharmacist led service could remove the need for Consultant follow up appointments and reducing waiting lists if effective and acceptable to patients, although the effect on waiting lists is yet to be evaluated.
Objectives
1. To evaluate the clinical effectiveness of the pharmacist led approach
2. To ascertain patients' perception of consultation with a pharmacist rather than a "specialist".
Methods
A postal questionnaire was sent to all patients seen by a pharmacist in the IBS Clinic. These patients were compared with a similar number of patients seen by a Gastroenterologist (and not the pharmacist) in order to compare the new approach with the traditional using the same questionnaire. Patients who did not respond were followed up by a telephone interview consisting of the original questionnaire.
Results
Patients in both groups reported improvements in the frequency of their symptoms (56% in study group, 42% in the control group). More patients in the study group felt their daily routine were interrupted less (44% compared with 29% in the control group). They were also using primary health care resources (GP and community pharmacist) less frequently after they had attended an appointment. Severity of symptoms was reported to be less after attending appointments with 64% of patients in the study group feeling their symptoms had improved compared with 58% in the control group, with higher proportion in the study group reporting their symptoms had improved "a lot".
Patients were happy to see a pharmacist rather than a Doctor, and patients who were initially unsure before their appointment were happier afterwards. Patients also preferred the longer appointments and felt they had had enough time to ask questions. Of the patients in the control group (who had had no previous contact with the pharmacist led approach), 83% felt that seeing a pharmacist for their symptoms would have interested them, with 17% unsure. No patients in the control group said they would not be interested in seeing a pharmacist.
Discussion
Patients attending the Pharmacist led clinic, showed a reduction in; symptom frequency, severity, use of primary health care resources and amount that symptoms impacted on daily routine. This demonstrated that this approach to management of IBS symptoms is at least as effective as the traditional methods and may be slightly more effective from a global symptom frequency viewpoint. However, this is difficult to quantify due to the lack of specific clinical endpoints.
Patient satisfaction is an important outcome measure and may be a predictor of patient concordance with therapy and higher levels of clinic re-attendance3 so it is therefore important the pharmacist led approach is acceptable to patients. There is evidence that certain categories of patient satisfaction such as provision of information and improved communication are positively related to health outcomes3, which may be especially pertinent in IBS patients in whom there is a high placebo response rate. The study group was successful in that patients felt involved in the decisions made regarding their treatment. It has been suggested that this should be the case as this leads to a degree of informed consent to treatment options and therefore informed choice for patients4. This is beneficial in that it enables a practitioner-patient relationship to develop that has been advocated in IBS1.
Pharmacists have been used successfully in the outpatient management of other disorders but there have been no reports in symptomatic management of IBS. Pharmacist involvement in outpatients to date has mainly been in monitoring and adjusting therapy that has already been started by another clinician, usually a doctor. This approach was novel in that the pharmacist was involved with making an assessment and initiating symptomatic relief accordingly. Prescribing privileges were necessary using the framework of an independent prescriber (Consultant Gastroenterologist) and a dependant prescriber (Pharmacist) authorised to prescribe certain medications within agreed plan as advocated by the Crown report5. The positive results of this study indicate that pharmacists are able to make clinical judgements based upon patients presenting symptoms and are able to initiate effective therapy based upon this clinical judgement, whilst involving the patient in these decisions to improve outcomes. The results of this study also agree with the recommendations of the Crown report that Pharmacists are a group of health care professionals capable of taking on the responsibility of prescribing in certain circumstances5.
References
1. Maxwell PR, Mendall MA, Kumar D. Irritable Bowel Syndrome. Lancet 1997;350:1691-5
2. Patee PL, Thompson WG. Drug treatment of the irritable bowel syndrome. Drugs 1992; 44(2): 200-6
3. Fitzpartick R. Surveys of patient satisfaction: 1 - important general considerations. BMJ 1991; 302: 887-9
4. Cleary PD, Edgman-Levitan S. Health care quality - incorporating consumer perspectives. JAMA 1997; 278: 1608-12
5. Crown J. Review of prescribing, supply and administration of medicines. Final Report March 1999
Evaluation of a Continuing Professional Development project for hospital pharmacists
Claire Grout
Oxford Radcliffe Hospitals NHS Trust
Introduction
The Berkshire and Oxfordshire Continuing Professional Development (CPD) project was established in December 1998 as an aid to recruitment and retention, and to support clinical governance requirements.1
A CPD portfolio was developed from interviews with a number of pharmacists and was refined following a pilot study.2 Each pharmacist develops their portfolio by reflecting against criteria and considering their job description, objectives, and personal plans. Records are made of achievements, how training has helped them to improve their practice, and what their current and future development needs are. In discussion with the CPD pharmacist, a personal development plan (PDP) is put together, taking into account the individual's learning preferences and availability of training opportunities. This is approved and items prioritised with the line manager. The whole process is ongoing.
Objectives
To obtain the views of pharmacists and managers regarding the CPD project.
Method
A questionnaire was sent to all pharmacists who had been included in the project and who were still employed in the two counties at the time of evaluation. The questionnaires were anonymous but were coded by department, as site feedback had been requested.
A separate questionnaire was sent to managers (chief pharmacists, departmental managers, and team leaders as appropriate).
Results
Pharmacists' responses (46/79 questionnaires returned = 58% response rate)
- 74% of pharmacists had achieved at least some of their planned development outcomes. The major barrier identified was lack of time.
- The discussion with the CPD pharmacist was found useful by 93% of pharmacists with the other 7% not sure.
- Only 20% of pharmacists updated their portfolio on a regular basis - most only 'occasionally' or 'when prompted'. Less than a quarter of pharmacists would continue to record their CPD if there was no follow up by a mentor, and many of these only if they had to.
- The preferred mentor was the CPD pharmacist (65%) and many commented on the independence of this role being beneficial. However 20% of pharmacists would prefer their line manager to be their mentor, 6% another colleague from their own department, and 9% a colleague from another department.
- 35% said that the project would encourage them to stay in post and 46% were not sure, many commenting that there were other factors to be considered.
Managers' responses (11/15 questionnaires returned = 73% response rate)
- 64% had seen definite outcomes from the project.
- 82% found that the project linked well with appraisal, although it was noted that these aspects should be seen as separate but complimentary.
- 45% thought the project was a useful tool in recruiting and retaining staff with a further 36% unsure, many saying it was too early to tell.
- A number of pharmacists and managers made suggestions for improvement to the project. These were largely related to the CPD pharmacist's time allocation for each Trust, and the possible involvement of more mentors in order to support the project.
Discussion
Evaluation demonstrated that the project could be a useful staff retention tool, which is extremely valuable in the current climate. It is encouraging that outcomes had been achieved for most pharmacists, although time for staff development must be made available to maximise benefit from a project of this type.
Meetings with the CPD pharmacist were valued, and it is of particular importance to note that individuals may be unlikely to continue recording their CPD without prompting by a mentor. In view of the fact that recording of CPD is likely to become mandatory for continued registration,3 the need for mentors to support the process could be vital. A number of mentors have subsequently been trained to aid continuation of the project.
Further analysis of outcomes of the pharmacists' CPD is being performed.
Acknowledgments
Grateful thanks to all the pharmacists who completed questionnaires, to the project steering committee (especially Jenny Dorey and Jane Hough who established and managed the post), and to the Berkshire & Oxfordshire Education Consortium for their financial support.
References
1. Department of Health. A First Class Service: Quality in the new NHS. HSC 1998/113. London. Department of Health. 1998
2. Grout C, Dorey J, Hough J. Continuing professional development for pharmacists: a strategic approach. Pharm J 1999; 263: R71
3. Royal Pharmaceutical Society of Great Britain. Society consults on disciplinary reform and competence-based practising rights. Pharm J 2001; 266: 220
To Glove or not to Glove...........that is the question
Hiom S.J.
St Marys Pharmaceutical Unit, Penarth, Wales, U.K.
Introduction
Good Manufacturing Practices (GMP) recommend the achievement of different environmental microbial standards at various phases in the preparation of Pharmaceutical products.To assist in this, operators are requested to follow SOP's relating to personal hygiene, including handwashing and donning of gloves. Hospital pharmacy production units across Wales currently adopt various handwashing protocols together with inconsistent approaches relating to which operations require the use of sterile or non-sterile gloves or indeed no gloves at all. Other healthcare professionals also experience difficulty in adopting a consistent approach to the appropriate use of sterile and non-sterile gloves1. Glove use issues involve cost, operator safety and contamination control. In order to make an informed decision and standardise SOP's across Wales, the microbial effect of commonly used handwashes and the bioburden of non-sterile gloves needs to be investigated.
Objectives
Determine the effect on hand bioburden of four commercially available handwashes.
Compare this with the bioburden of non-sterile gloves
Method
Three fingers from each hand (excluding thumb and little finger) were placed in contact for 3sec with D/E Neutralising agar before and immediately after handwashing.The handwashing instructions were followed on each of the four commercial products: Levergel, Hydex, Hibiscrub and Videne and the hands subsequently fan dried.The same individual was used throughout the experiment using a different handwash each day, the order randomised using latin square methodology.
Each handwash was tested five times.The plates were incubated at 30C for 48 hrs and then counted for colony forming units (cfu).Soap and water (n=5), and mechanical rubbing of hands without water or chemicals (n=5) were used as controls.The above method was also used to test the surface bioburden of non-sterile, powder free, latex gloves (n=5).Contamination of the water supply used for washes was determined.
Results
Non - sterile gloves 0 cfu per finger dab (n=5)
Tap water contamination 70 cfu/ml
Fig 1 CFU per finger dab before and after handwashing
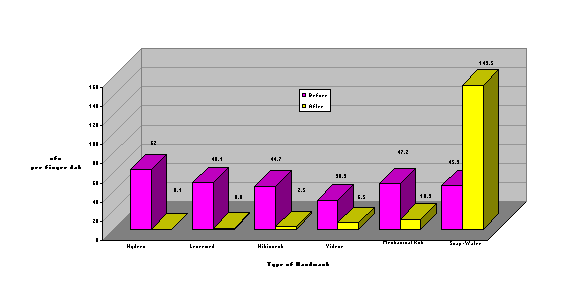
Discussion
In this study soap and water increase the surface bioburden of washed hands by approximately three fold. This may be due to a movement of commensal organisms from finger grooves to the surface of the skin.Mechanical rubbing of the hands, for one minute, reduced surface bioburden by approximately 80%. With the exception of Videne, all commercial products tested were statistically (p=0.1) more effective at reducing hand bioburden than mechanical rubbing of hands. No significant difference (p=0.1) was shown between the remaining products tested - Hydrex, Levermed and Hibiscrib.When comparing products, local water contamination must be taken into account. Levermed is the only product not requiring water and hand drier facilities2. Non-sterile gloves showed no contamination using the finger dab approach. Cost considerations may substantiate the use of non-sterile gloves, instead of sterile gloves, for activities outside the controlled work zones. However, previous work3 and preliminary work by the author, using a total immersion technique4, showed contamination of non-sterile gloves of approx 4 and 8 cfu/glove respectively. Further work to examine 'total' contamination of non-sterile gloves is in progress. Contact contamination remaining on hands immediately after washing with either Hydrex, Levermed or Hibiscrub was demonstrated to be low (1.1 + 1.0 cfu/finger dab). In working areas outside the controlled work zone and where operator safety has been assessed, the use of surgically scrubbed bare hands may be acceptable. Further work, however, to examine the disinfection duration of reduction in bioburden on the hands is in progress.If non-sterile gloves are to be used in critical operations the bioburden of each new batch can be tested, prior to use, with this method.
References
1. O'Toole, S. Disposable gloves. Professional Nurse. 1997, Vol 13, 184-190.
2. Voss A, Widmer AF. No time for handwashing!? Infection Control Hosp Epidemiol, 1997 Mar, 18:3, 205-8.
3. Rossoff, LJ et al. Is the use of boxed gloves in an ICU safe? Am J Med 1993, Vol 94, 602-5
4. Hiom, SJ. R+D Report - Welsh Pharmaceutical Services. Bioburden of Sterile vs non-sterile gloves. 1999.
South West Pharmacy Assistant Accredited Training Scheme
Cousins A
South West Medicines Information and Training, Bristol Royal Infirmary, Bristol
Introduction
The NHS plan has highlighted the need to re-organise health services to improve patient care and make better use of resources 1.
In addition, the recently published pharmacy programme - Pharmacy in the Future and the consultation document - A Health Service of all Talents have made more specific references regarding the need to develop the role of the pharmacist in the prescribing and medicines management agenda 2,3.
However the National Health Service Pharmacy Education and Development Committee 1999 national survey reported that due to the present shortage of pharmacists and technicians, intended pharmacy services have been curtailed in half of the hospitals in Britain 4.
Therefore to achieve the aims outlined in the pharmacy programme better use of all pharmacy staff will be required (2). Adequately trained support staff working to safe operating procedures could allow services to be re-organised in a more efficient manner, with the potential to add value and provide additional services 5.
The need to develop a qualification to ensure the adequate training of support staff has been recognised for some time 5.
This paper outlines the approach taken in the South West to preparing a scheme to assist with the training and development of support staff.
Objective
To develop a regional training scheme for pharmacy assistants.
Method
Job descriptions for support staff were requested from all trusts within the region and a summary of key roles performed by pharmacy assistants prepared. Five key roles were identified . All activities involved in each process were mapped to assess:
- the most appropriate staff group to perform each activity,
- the underpinning knowledge necessary to perform the role competently.
Results
The outcome of this process lead to a framework of activities that pharmacy assistants could perform. A competency based training scheme was then developed. The format of the documentation was based on the current standard format of units in the National Vocational Qualification in Pharmacy Services Level 3. The five key roles identified for pharmacy assistants became the training unit titles.
Table 1: Units in South West Pharmacy Assistant Accredited Training Scheme
Dispensing
Aseptic Preparation and Dispensing
Distribution and Top-up
Stock Management
Pre-packing and Over-labelling
Five units were prepared, in each unit there are several elements, which represent the consecutive activity within the role. Each element contains performance criteria, range statements, underpinning knowledge requirements and evidence requirements.
Discussion
The preparation of the scheme has demonstrated that a high quality training scheme can be produced by following this logical process.
In a six month period, 32 pharmacy assistants have registered to participate in the training scheme demonstrating that Pharmacy assistants are willing to develop their knowledge and skills and gain formal recognition of their training.
Acknowledgements
The author acknowledges the help and support given by:
- South West Medicines Information & Training Department: Trevor Beswick, Lynne Bollington, Deborah Marriott, and Deborah Ford,
- The Assistant Advisory group: Jane Foster, Robert Padbury, Jane Rogers, and Jayne Worth,
- All other specialist pharmacists and technicians from the region who contributed to the training scheme
- Pharmacy Assistants who have participated in the scheme.
References
1. The NHS Plan, Department of Health, 2000
2. Pharmacy in the future- Implementing the NHS Plan, Department of Health, 2000
3. A Health Service of all the talents: Developing the NHS workforce, Department of Health, 2000
4. Pharmacist shortages curtail services at half of Britain's hospitals, Pharm J, 2000; 264:866
5. Making the best use of pharmacists and their support staff, Pharm J, 1998; 260:743-745
Availability and Appropriateness of Medicines Information for the Paediatric Population
Paula Hayes1, Andrea Gill1, Catherine Murphy2, Hannah Thorpe2
1 RLCH NHS Trust, Alder Hey, Liverpool, 2 Liverpool John Moores University, Liverpool
Introduction
On 1st January 1994 "The Medicines for Human Use (Marketing Authorisations etc.) Regulations" came into force. As a result since 1st January 1999 it has been a legal requirement for all medicines to be supplied with a patient information leaflet (PIL). The implications for hospital pharmacists are that PILs should be provided with all medicinal products supplied to outpatients, discharge patients and inpatients.1 The availability of PILs with manufacturers' packs varies considerably. For a number of preparations further copies must be obtained or photocopies made - the latter may breach copyright regulations. The problem is further complicated in paediatrics where many medicines are unlicensed or used off-label - in these cases manufacturers' PILs are inappropriate (ie contain disclaimers such as 'not suitable for children'). The Pharmaceutical Society have stated that they will not defend a pharmacist who fails to comply with the regulations, nor will they defend them against a claim for damages if harm results from the pharmacist's failure.2 In light of the legal and ethical implications surrounding the supply of PILs it was decided to undertake a review of the practices at RLCH NHS Trust, Alder Hey Pharmacy Department. PILs are supplied on an ad-hoc basis to outpatients and discharge patients and there is currently no system in place that allows inpatients access to PILs.
Aims & Objectives
- To assess the availability of PILs (including 'in house' leaflets) for medicines supplied from the pharmacy and to determine their appropriateness for the paediatric population.
- To investigate the supply of PILs (including 'in house' leaflets) to discharge patients and determine reasons for not supplying.
- To make recommendations to the Trust on methods of improving the provision of PILs and the resources to do so.
Method
An 'Access' database was set up to collate data about the availability and appropriateness of manufacturers' PILs. The data collected included:
- Drug name, strength & form
- Manufacturer
- Availability of PIL
- Appropriateness of PIL for paediatrics
- Other relevant comments
For a one week period all 'TTO' prescriptions were reviewed in order to determine the number of items issued without a PIL and to ascertain the reasons for this (due to time constraints only tablet, capsule and liquid formulations were reviewed). An audit undertaken in 1998 had shown that 82% (n = 302) of 'TTO' prescriptions were supplied without a PIL - had there been any improvement?
Results
Availability and appropriateness of manufacturers' PILs (for tablet, capsule and liquid formulations)
Data was collected for 430 preparations (223 different drugs). This comprised 322 tablet and capsule formulations and 108 liquid formulations. The availability of a PIL for the solid dose forms was; a leaflet available & suitable for paediatrics (41%) a leaflet available but unsuitable for paediatrics (32%) and no leaflet available for 27% of these formulations. The availability of a PIL for liquid formulations was; a leaflet available & suitable for paediatrics (61%), a leaflet available but unsuitable for paediatrics (5%) and no leaflet available in 34% of these formulations.
Table 1: Supply of PILs with TTO medicines
| Items dispensed (n=268) |
% |
| Items supplied with a manufacturer's PIL
|
41 |
| Items supplied with an 'in house'
|
6 |
| Items supplied without a PIL
|
53 |
Discussion
The results show that the availability and appropriateness of manufacturers' PILs is a problem in the paediatric population. More than half of the tablet, capsule and liquid preparations supplied from the pharmacy department do not have a manufacturers' PIL or the PIL is not suitable for children. The majority of discharge patients (74%) receive at least one medicine without a PIL and almost a third are not given PILs for any of their medicines. The reasons for not supplying PILs are limited. Multiple dispensing from large dispensing packs with only one PIL and having PILs attached to original bottles which are inappropriate to dispense account for over half of the items and lack of availability or inappropriateness accounts for about a quarter of the items. In 17% of cases a leaflet was available and appropriate but not supplied - this shows that there is still a need to educate staff about supplying PILs. Since the 1998 audit there has been an improvement in the supply of PILs with "TTO" items. This is the result of educating pharmacy staff about legal and ethical requirements around provision of PILs. The Royal College of Paediatric and Child Health (RCPCH) and the Neonatal and Paediatric Pharmacist Group (NPPG) have recognised this problem and are designing two generic PILs (one for children and one for parents) to explain why it is sometimes necessary to prescribe unlicensed medicines or to use licensed medicines for unlicensed indications.
Conclusion
The supply of PILs with all medicinal products to discharge patients, outpatients and inpatients is a legal requirement. At RLCH NHS Trust 54% of tablet, capsule and liquid formulations do not have an available or appropriate PIL and 53% of 'TTO' items are supplied to patients without a PIL. There is no system to allow inpatients access to PILs. We have proposed the following recommendations that will improve the provision of appropriate PILs to all paediatric patients at RLCH NHS Trust.
- Develop the database to include information about all drugs and all formulations and to update and review on a 6 monthly basis.
- To continue to raise awareness among pharmacy personnel about the importance of supplying PILs to discharge patients and outpatients.
- To implement the use of the RCPCH / NPPG leaflets when available.
- To review 'in house' information leaflets by developing a standard format which complies with legal requirements and preparing information for drugs commonly supplied without PILs.
- To investigate and develop a system for inpatients to have access to PILs at ward level.
A report will be presented to the Trust.
References
1. Royal Pharmaceutical Society of Great Britain, Professional Standards Directorate Fact Sheet Three: The Medicines for Human Use (Marketing Authorisations etc) Regulations 1994, and the Effect Thereof.
2. The Pharmaceutical Journal, Vol 264 No 7091 p544 (letters): Disappointed and Dismayed.
Intravenous drug use in the Intensive Care Unit (ICU)
Chris Cairns, and Fozia Mushtaq
University Hospital Lewisham, London SE13 and King's College, University of London. London, SE1
Introduction
Research has shown that transferring the preparation of IV doses from ward based nurse preparation to pharmacy centralised intravenous additive services (CIVAS) is associated with a number of benefits. These include improvements in the timeliness of dosing1,2,3 and significant economic advantages1,2,4,5,6. This work has been carried out for both adults 1,2,4,5 and children6 but not in critical care. . Extensive use is made of the IV route in ICU. Apart from one piece of work2, which has significant limitations, there is little evidence of either economic benefit or even an indication of workload in ICU. It is, therefore, important to obtain, initially evidence on the level and nature of IV drug use in British ICUs and then carry out some robust economic analysis. The study described here addresses the initial task of characterising and quantifying the present workload in a busy ICU in a University Hospital.
Objectives
- To identify the agents given by the IV route and their dosage.
- To quantify the number of IV doses of drugs given.
- To identify the incidence of the differing methods of drug administration.
- To identify the nature and volumes of diluents.
- To quantify the mode of administration.
- To model the effects of this workload on nurse time.
Method
The study was carried out over a four week period in a 9 bedded ICU. Four days a week each patient's drug charts, ICU flow charts and notes were reviewed by a single researcher. IV doses since the last data collection were identified and information for each dose abstracted: drug, dose of drug, volume and nature of diluent, mode of administration (e.g. syringe driver, burette, etc.) and method of administration (bolus, intermittent, continuous). Ambiguities and missing information were clarified by discussion with the nurse caring for the patient and/or direct observation. All doses from admission to discharge or death were recorded. Patients who had been discharged or died between data collection episodes had their notes retrieved and data abstracted. Doses that were administered epidurally were included but all other routes e.g. into haemofiltration circuits were disregarded, as were IV fluids for rehydration and/or fluid resuscitation. Data were collated and analysed using Microsoft Excel. Modelled implications in nursing time were calculated by using the mean time to prepare a dose from 3 studies [8], [9], [10]. Potential costs were derived by applying nurse salaries (grade E and F) to this data.
Results
Thirty one patients were admitted accounting for 2129 IV doses and 11 epidural doses. The commonest drug administered IV was Ranitidine; 444 doses (21%) followed by Metronidazole; 236 (11%) and Cefuroxime; 103 (5%). 10 drugs accounted for 60% of all doses. A third of doses, 727 (34%) were given by bolus injection, 853 (40%) by intermittent infusion and 548 (26%) by continuous infusion (including the 11 epidural doses). Six drugs accounted for 80% of all bolus doses, Ranitidine, Amoxycillin, Ceftazidime, Cyclizine, Sodium Valproate and Cefotaxime. Intermittent infusions were given in minibags in 709 (83%) occasions, mainly in 100 ml bags, in the original bottle 50 (6%) and via a burette system on 94 (11%). In addition to those drugs administered from the original bottle, there were 236 doses of Metronidazole and 78 doses of Ciprofloxacin given from original containers.
A syringe driver was used for all but two of doses given by continuous infusion. 85% of doses (454) given were accounted for by 11 drugs. The commonest drug given by continuous infusion was Dopexamine; 92 doses, followed by Morphine; 51 doses and Noradrenaline; 46 doses. Overall 2 IV doses (0.1%) were given in large volume infusions (500 ml or greater), 535 (25%) via syringe pump, 1487 (70%) in small volume infusions and 94 (4%) via a burette. Twelve drugs accounted for 60% of all doses administered.
The modelled cost in nurse time to prepare these doses varied between 79 (Wilson 4) and 126 (Plumridge et al 5) hours per week. The financial cost of this in nurse salaries varies between £767 and £1,386 per week depending on grade and the research work used. These equate to between £39,860 and £72,070 per annum respectively. These costs are the mid points of the E and F grade scales and do not include London Weighting or unsocial hours payments.
Discussion
The number of doses prepared and administered was high, over 500 a week. The actual amount will be greater as the analysis did not include additions to haemofiltration bags and drugs administered into haemofiltration circuits. This workload consumes a lot of nurse time, depending on what study is used to determine time for preparing a dose, varying from 79 to 128 hours per week. This equates to between 2.26 and 3.67 Whole Time Equivalents, or approximately one nurse at any one time, assuming 3 shifts per day. This is a major cost implication, although not all may be realisable if the work was transferred to a CIVA service. A relatively high volume of the workload comes from a limited number of drugs and there was considerable consistency of dosages employed of individual drugs. This would ease the transfer to CIVAS as doses could be prepared to standard strengths rather than being dispensed individually to a variety of strengths, volumes and dosage forms.
Conclusions
The number of IV doses given on an ICU is high and preparation represents a significant resource implication for nursing staff. Although the number of doses is high, over 500 a week, 60% of all doses are represented by 10 agents.
References
1. Clarke C et al, Parenteral drug delivery - value for money? Pharm J. 1986; 236: 453-455.
2. Cannon J, Bertch K, Cousins D. The introduction of a satellite pharmacy service for the intensive care and coronary care units at a district general hospital. Pharm J. 1990; 244: HS36-39.
3. Davey P et al. Audit of IV antibiotic administration. Pharm J. 1990; 244: 793-795.
4. Wilson M. An evaluation of the cost effectiveness of a centralised intravenous admixture service. Proceedings of the Guild. 1990; 27: 3-11.
5. Plumridge R and Maher M. Justification of a pharmacy intravenous admixture service in an Australian hospital. Am J Hosp Pharm. 1993: 50: 463-466.
6. Armour D, Cairns C, Costello I, Davies E, Riley S. The economics of a pharmacy based central intravenous additive services. Pharmacoeconomics. 1994; 10: 386-394.
Intervention Monitoring in the Dispensary
Chris Cairns and Yee Mei Yau
University Hospital Lewisham, London SE13 and King's College, University of London, London SE1
Introduction
Interventions monitoring has long been an integral part of ward based clinical pharmacy activities.1,2,3 It is viewed by many senior pharmacists as an important clinical governance activity, and can be used to improve prescribing quality.1,4 Further uses include demonstrating pharmacists' contribution to patient care2,3 measuring cost savings,3 and as a peer review tool.3,4 However, its use has been confined to ward based activities and interventions which occur in the pharmacy, particularly in the dispensing process, ignored. Dispensing of medicines is a clinical activity where steps in the medicine use chain2 are important. Interventions occur within the dispensary yet no work has been published on any aspect of them, number, nature or importance. This study was set up to determine the frequency and nature of pharmacists' intervention in a busy hospital pharmacy dispensary.
Objectives
- To identify the number of interventions carried out in the dispensary
- To determine the nature of these interventions.
- To measure the impact of interventions on patient care.
Method
The study was carried out three days a week over four weeks, following a one week pilot. Copies of outpatient and A&E prescription forms were reviewed frequently during the day and interventions identified from pharmacy staff endorsements. Data were abstracted from the prescription, the relevant pharmacist or technician approached and the remainder of the details of the intervention recorded. Interventions data on discharge prescriptions (TTOs) were collected by direct observation by the researcher at the TTO workstation. Inpatient orders were excluded as the vast majority of the work had been pre-screened by a pharmacist on the ward.
Data collected were based on that described in the literature,5 including origin of the prescription, type of problem, reason for intervention, outcome, time taken and a brief description of the intervention. A list of definitions and examples were drawn up in advance of data collection to aid consistency of data collection. Each intervention was given an acuity score2. This was assigned by the researcher at the time of recording and reassessed during the analysis. A sample of acuity ratings was independently assessed by one of the clinical pharmacists and correlated against the researcher. Data were analysed using Excel. Baseline workload data was generated from the pharmacy computer system.
Results
278 interventions were recorded, 170 on outpatient/A&E prescriptions and 108 on TTOs. The overall rate was 4.6%; outpatients/A&E 5.6% and TTOs 3.8%.
The commonest outpatient interventions were for A&E, 34 (20%), followed by Paediatrics, 18 (11%), Dermatology, 16 (9%), Paediatric A&E, 14 (8%), Psychiatry, 11 (7%) and General Surgery, 10 (6%). A third of these were dosage discrepancies, 57 (34%), then Rx illegible/ ambiguous/incomplete 43 (25%), as broken down in Table 1. The main reason for intervention was safety, 53 (31%), cost saving, 40 (24%), patient care, 34 (20%) and effectiveness 33 (19%). The prescription was changed by the pharmacist following guidelines, etc., 59 (35%) and 58 (34%) following contact with a doctor, while 16 (9%) were information only. Half were considered 'standards of practice', 93 (54%), 35 (21%) were of 'financial significance' and 9 (5%) each 'prevented drug toxicity' and 'changed sub therapeutic dose'. 24 interventions were the provision of 'information only'.
Commonest TTO interventions arose on charts from Medical wards, 32 (30), Surgery, 29 (27%), Paediatrics, 26 (24%) and Obstetrics 9 (8%). Dosage discrepancies were commonest, 22 (20%), then Rx illegible/ambiguous/incomplete 18 (25%) with drugs omitted or duplicated on 14 (13%) occasions each, as broken down in Table 1. The main reason for intervention was patient care, 46 (42%), safety, 24 (22%), cost saving, 17 (16%) and effectiveness 10 (9%). The prescription was changed by the pharmacist following guidelines, 48 (44%) and 33 (31%) following contact with a doctor, while 12 (11%) were information. Two thirds were considered 'standards of practice', 73 (68%), 16 (15%) were of 'financial significance', 4 (4%) 'prevented drug toxicity' and 3 (3%) 'changed sub therapeutic dose', with 12 provision of 'information only'.
Table 1 Types of intervention
| Type of Problem |
Outpatients (%) n=170 |
TTOs (%) n=108 |
| Dose/frequency |
57 (34) |
22 (20) |
| Rx illegible/ambiguous/incomplete |
43 (25) |
18 (17) |
| Drug omitted |
0 |
14 (13) |
| Drug duplicated |
1 (1) |
14 (13) |
| Non formulary |
26 (15) |
2 (2) |
| Duration |
13 (8) |
5 (5) |
| Drug availability/supply problem |
8 (5) |
7 (7) |
| Rx illegal |
5 (3) |
9 (8) |
| Choice of drug |
5 (3) |
4 (4) |
| Formulation/route |
5 (3) |
9 (8) |
| Other |
7 (4) |
4 (4) |
Discussion
This work shows a significant number of interventions take place in the dispensary with a rate approaching 5%. Although multiple sources the high incidence of A&E interventions highlights an area for attention. Paediatrics is also of note, in both outpatients and TTOs. TTOs are very significant as although intervention numbers in paediatrics is similar to medicine and surgery the number of wards are 2, 9 and 7 respectively. Many changes were made by pharmacists acting on devolved responsibility, and few interventions were not changed by doctors.
Conclusion
A significant number of interventions take place in a hospital pharmacy dispensary. Particular attention should be paid to prescriptions from A&E and Paediatrics.
References
1. Hawkey C et al. Effect of reactive pharmacy intervention on the quality of hospital prescribing. Br Med J. 1990: 300: 986-90.
2. Cousins D, Hatoum H. The development of a computerised quality assurance system for clinical pharmacy. Int J Pharm Prac. 1991; 1: 86-9.
3. Hubbard G, Alder G, Interventions during prescription checking on ward rounds. Pharm J. 1992; 248: 162-3.
4. Barber N, Batty R, Ridout D. Predicting the rate of physician-accepted interventions by hospital pharmacists in the UK. Am J Health-Syst Pharm. 1997; 54: 397-405.
5. Barber et al. Consensus statement on a minimum data set for hospital pharmacy prescription monitoring events. Pharm J. 1992; 249: 346.
The unlicensed use of oral ketamine - provision of information to General Practitioners and patients
Webb E.J. 1, Alldred A. 1, George B. 1, Wright D 2.
1 Pharmacy Department, Leeds General Infirmary and 2 School of Pharmacy, Bradford University
Introduction
The use of oral ketamine to treat chronic pain is a relatively new concept. There are a number of published case reports and small trials detailing the success of ketamine in this area, but as yet no large randomised controlled trials. 1,2 Ketamine is only available as an intravenous formulation. Oral ketamine for the treatment of chronic pain is an unlicensed indication. Concerns from GP's have arisen in Leeds due to very little prescribing information being supplied to primary healthcare professionals.
This paper describes the production of information to ensure the safe and appropriate continuation of oral ketamine in primary care.
Objectives
- To identify the information requirements of primary care prescribers
- To identify the most appropriate method of information dissemination
- To develop appropriate information to ensure safe prescribing of oral ketamine
Method
From a retrospective prescribing audit we identified fifty patients receiving oral ketamine therapy for chronic pain. Analysis of pain clinic medical notes identified twenty-five patients whose GP had been asked to continue prescribing ketamine. All twenty-five GPs were sent a questionnaire with a covering letter. The questionnaire attempted to identify what prescribing information, if any, had been provided from the hospital. This survey included questions such as: awareness of unlicensed status, indication for use, dosing schedule, adverse effects, monitoring requirements, treatment costs and future management plan. GPs were then asked what further information they required to enable safe prescribing of oral ketamine and how this could best be communicated. Pre-paid envelopes were provided and GPs were asked to reply within one month. Non-responders were followed-up with a single telephone call.
A patient information leaflet (PIL) and prescribing information sheet were updated and developed as a result of the response from GP's.
Results
From the twenty-five GPs surveyed, twenty-one (84%) responded, either in writing or by telephone interview. One respondent had not been approached regarding this matter and was therefore excluded from the analysis.
GP knowledge of ketamine prescribing information varied. Fifteen respondents were aware that oral use of ketamine for chronic pain is an unlicensed indication, however five were not. Although the majority of GPs understood the indication for use, only six were aware of the possible adverse effects and only two knew the specific monitoring required. The cost of treatment was only appreciated by five out of twenty GPs.
Table 1. Results of GP questionnaire identifying awareness of ketamine prescribing information.
| |
Number of GPs aware of prescribing information |
| Prescribing information |
Yes |
No |
| Indication for use |
18 |
2 |
| Dosing schedule |
16 |
4 |
| Adverse effects |
6 |
14 |
| Monitoring required |
2 |
18 |
| Aware of unlicensed use |
15 |
5 |
| Cost of treatment |
5 |
15 |
| Future management plan |
7 |
13 |
Fifteen out of the twenty (75%) continued to prescribe ketamine; five did not. The main reasons given for refusing to prescribe ketamine were the unlicensed status of the drug for this indication and the lack of access to necessary prescribing information.
All respondents stated they would value an information sheet providing ketamine prescribing information.
A basic data sheet had previously been developed to send to GPs and community pharmacists via the patient. From the results of this survey it is clear that the information included was insufficient. Sending important information via the patient was inappropriate and an unreliable means of communication. The existing GP data sheet was therefore amended to include all areas addressed in the questionnaire. The information is now sent with the clinic letter directly to the GP. A patient information leaflet (PIL) was also developed from the response to the survey and has been well received by patients. This leaflet is provided with a manufacturers PIL in order to meet EEC legislation.
Discussion
GP knowledge of ketamine prescribing guidance varied greatly. Twenty five percent of GP's asked to continue ketamine therapy felt unable to do so because of a lack of information. This study has identified a need for information provision to ensure the safe use of oral ketamine in primary care. It also identified the requirement for a robust and appropriate means of communication. The review of the existing GP information leaflet, and the development of a PIL have facilitated a shared care approach to the management of these patients. Recent feedback has suggested an overall improvement in the management of patients receiving oral ketamine.
References
1. Nikolajsen L, Hansen P, Jensen T. Oral ketamine therapy in the treatment of
postamputation stump pain. Acta Anaesthesiol Scand 1997; 41:427-429
2. Hoffman V, Coppejans H, Vercauteren M, Adriaensen H. Successful treatment of post-herpetic neuralgia with oral ketamine. Clinical J Pain; 10(3): 240-2
Inappropriate Secondary Care Prescribing of PPIs has a Significant Influence on Primary Care: Fact or fiction
Beckett R, Conroy C, Cattell R
Department of Pharmacy. Bristol Royal Infirmary. United Bristol Healthcare Trust
Introduction
During hospital admission new therapy in initiated and stopped. Any new therapy that the patient is discharged upon is likely to be repeatedly prescribed adding to the burden of cost to the primary care group/trust. The effect of secondary care prescribing on the cost of primary care medicines expenditure has been studied widely and remains a source of debate at interface meeting within the NHS.
The UBHT Drug Interface Group (DIG), a committee of PCG prescribing leads, drug and therapeutic representatives and clinicians, discusses the introduction of new medicines which will be prescribed mainly in primary care and any issues surrounding the use of medicines across the interface. The expenditure of approximately £5.4M (p.a.) on proton pump inhibitors (PPIs) within Avon is growing at around 10% per annum and so following the recent NICE guidance, the Group agreed to examine the prescribing of PPIs within the Bristol Royal Infirmary (BRI).
Objective
To identify the point of prescribing in secondary care and to consider its appropriateness.
Method
Two hundred consecutive patients admitted through the medical admissions unit (MAU) were included in this study. They were identified on admission and tracked throughout their hospital stay and then reviewed on discharge. Consecutive admissions were used to eliminate bias.
A data collection form was developed and piloted prior to the study. The four distinct sections.
Demographics: An addressograph (name, DOB, number ) was used for speed and clarity.
Section 1 is completed if the patient was taking a PPI on admission
Section 2 is completed if the PPI was commenced as an in-patient
Section 3 analyses the discharge prescription
Results
During the month long recruitment phase two hundred patients were initially identified. Of these patients forty-two were lost to follow up and one hundred and fifty eight patients data was analysed. (82 male, 76 female)
The main data from this study is shown below
Table 1: Proton Pump Inhibitor Use in Patients admitted to the BRI via MAU
No PPI during admission
or on discharge
% (n) |
Taking prior to admission
% (n) |
R.I.P. during admission
% (n) |
Started during admission
% (n) |
| 70.8% (112) |
15.8% (25) |
8.8% (14) |
4.4% (7) |
Of the 7 patients who were prescribed PPIs during their admission. 4 (57%) were prescribed lansoprazole, which is the preferred PPI within UBHT and throughout Avon Health Authority. Omeprazole (2) and pantoprazole (1) were also prescribed. Of these 7 patients, only 1 was prescribed a PPI for no documented or evident reason. Helicobacter Pylori eradication (1) , endoscopy positive GORD (2), duodenal ulcer (1), dysphagia (1) and NSAID use in a high risk patient (1) were the indications in the remaining patients.
Discussion
This study provides clear evidence that whilst PPIs use remains high, the impact of inappropriate secondary care prescribing on primary care expenditure is not significant. It also highlights the need for better communication within the trust regarding PPI choice.
One area not examined in this study was the information given on discharge to primary care relating to the newly prescribed PPI. DIG should be encouraged to look further into this aspect of prescribing.
The use of a patient focus group to development a holiday travel information booklet for patients on lithium.
Janine Acomb
Pharmacist, Airedale NHS Trust. Yorkshire
Introduction
The pharmacy led lithium clinic has been running at Airedale General Hospital for over 8 years. It now has 130 patients registered with the clinic. The routine clinic visit involves patients having their 12 hour serum lithium level measured and then receiving dosage and other advice from a pharmacist. Monitoring of thyroid function, calcium levels and renal function is also carried out according to an agreed schedule. In addition the clinic runs "coffee mornings" every 4 - 6 months. These meetings allow a group of patients and carers to meet for fellowship and to discuss various aspects of their therapy. Over the years the clinic has received a number of enquires mainly from its own patients, but also from around the country, enquiring about potential problems with holiday travel whilst taking lithium. I decided to write an information leaflet and to use one of these coffee mornings as a patient focus group to identify issues and draw on patients' experiences.
Objectives
- To use a patient focus group to identify potential problems that patients taking lithium may experience whilst travelling abroad and to share experiences.
- To evaluate a draft booklet in a larger number of patients.
- To produce an information booklet.
Method
A patient focus group was set up by inviting all patients (excluding patients in nursing homes) and carers to a coffee morning. I then led a structured discussion on the issues. Patients and carers were asked about various problems envisaged by the pharmacist and then asked to identify other potential problems. Finally patients were asked to share good and bad experiences so that ideas and answers were shared. A record was made of the main points. A brief, anonymous evaluation sheet was given to each participant.
I used the information gained from the patient focus group to draft an information booklet. This draft booklet and a questionnaire was then sent to all registered patients (excluding patients in nursing homes) and to the consultant psychiatrists who refer patients to the clinic. This information was collated and is being used to write the final information booklet.
Results
Fifteen patients and carers attended the patient focus group. The patients and carers identified 25 issues compared to the 11 that I had identified. Six patients or carers filled in the evaluation form. All found the subject of the meeting 'very useful' or 'useful' and all found the meeting 'very enjoyable' or 'enjoyable'. All of the free text answers were positive and one patient stated that they had gained confidence from the meeting.
One hundred draft information booklets and questionnaires were posted to patients. Thirty-three patients returned the questionnaire. The questionnaire showed that patients found the booklet easy to understand and provided useful information (see Tablet 1). Eight patients made further suggestions or clarification of issues in their response.
Table 1. Patient evaluation of holiday travel booklet
| Evaluation statement |
Number of Patients responding |
| |
Strongly
agree |
Agree |
Disagree |
Strongly
disagree |
| The leaflet was easy to understand |
17 (52%) |
16 (48%) |
0 |
0 |
| The leaflet told me everything I wanted to know |
13 (39%) |
19 (58%) |
1 (3%) |
0 |
| The leaflet told me something new that I did not already know |
11 (33%) |
19 (58%) |
3 (9%) |
0 |
| I found the booklet format made it easy to find the information I wanted |
12 (36%) |
21 (64%) |
0 |
0 |
| I know where to find more information |
13 (39%) |
18 (55%) |
2 (6%) |
0 |
The draft booklet was sent to six consultant psychiatrists for comments. Two consultants responded with useful comments.
Conclusion
The main feature of this project was to involve of patients and carers in identifying and resolving issues. The methodology was successful with many patients feeling they had made a contribution to the booklet. The patient focus group confirmed many of the pharmaceutical issues that I had identified. They also identified a number of more general areas of concern that had not originally been identified. The evaluation by patients of the draft booklet was positive. The recent NHS plan emphasises the concept of empowering patients to take an active role in managing their own care1. I have developed a model of practice that promotes this policy. Patients are not passive recipients of prescribing and must be involved in their own care. When given an appropriate framework I have shown that patients are willing to become involved in medicines management. A final booklet is being prepared.
References
1. Paragraph 3.11 Pharmacy in the Future - Implementing the NHS Plan. Department of Health. September 2000
Re-engineering pharmaceutical care for Ear Nose and Throat (ENT) patients
Nadine Senner, Chris Cairns and Michelle Predki
Directorates of Pharmacy and ENT, University Hospital Lewisham, London SE13
Introduction
In general, ENT patients fall into one of two distinct categories. The majority of patients are short-term admissions, frequently overnight only. There are also a small number of patients, who have head and neck cancers and end to have prolonged admissions. The pharmaceutical care priorities for both groups differ dramatically. For the majority, all activity is led by their hospital stay which can be described succinctly as: admit, operate and discharge early next day to clear bed for next patient. Although a wide range of procedures and treatments are used, patients can be generally characterised: a high proportion of patients are young and on little or no regular medication, while those on regular medication rarely need it changed while admitted. They are ambulant within 24 hours and go home on some combination of analgesia, antibiotics and/or topical therapy. Patients with head and neck cancers conversely have prolonged admissions and require constant medication review and monitoring. A strong focus on medicine formulation is needed as much drug administration is via a nasogastric or a percutaneous feeding tube.
The existing service was based on traditional ward/clinical pharmacy service: i.e. twice daily visits, discharge scripts (TTOs) to pharmacy and inpatient supplies dispensed for a week at a time. For the short term patients this was not ideal as it led to delayed discharges, patients not returning for TTOs, missed inpatient doses and complaints from patients. The delivery of care was re-engineered to be responsive to these patients needs. This study describes the re-engineered care and it's evaluation.
Objectives
- To identify the effect of the new service on TTO dispensing.
- To quantify the number of interventions made and their effect.
- To identify the costs avoided in drug expenditure.
Method I - The new model
As the majority of the problems were centred around the discharge process this area was examined first. TTOs were reviewed and the common agents used on TTOs and their dosage identified. A TTO cupboard for ward based dispensing was set up with already labelled prepacks of antibiotics, analgesics and topical agents. Stock topical preparations for inpatient use were supplied with a pre-printed TTO style label. Patients' own drugs (PODs) are used for regular medication. The pharmacist's routine is to arrive on the ward first thing in the morning, during or immediately after the ward round and deal with the TTOs first. PODs are returned to the patient, and analgesia and/or antibiotics dispensed. Topical medications are first checked with the patient to see if they have already been issued with an inpatient supply. The inpatient supply is appropriately labelled or a TTO supply made. The TTO is bagged along with a copy of the discharge letter and a Medicine Hotline card. The patient and medicine details are recorded on a dispensing log. All patients going home that day are counselled on their medicines and issued with them by the pharmacist. Phase II of the process is now under way with the introduction of POD boxes and one stop dispensing for medium and long term patients.
Method II - Evaluation
Ward based dispensing numbers were abstracted from the ward dispensing log. During a one month period, before phase II, all avoided dispensing was recorded. Cost avoidance was calculated using hospital prices. All clinical interventions were recorded and analysed in the standard hospital intervention format, over a four week period. During the same period a record was made each time a patient was counselled on their medicine use.
Results
TTOs were dispensed in the ward for 336 patients, over a six month period. A total of 825 items were dispensed. Over 90% of these were dispensed and given to patients before 10.00 am. During the sample four weeks 44 patients were counselled on their medicines, this accounting for all patients, who had their TTO dispensed on the ward, except one. The mean was 2.2 patients each day, but the range was wide varying from none to 8. A total of 38 interventions were made on ENT patients, which corresponds to an annual estimate of 494. The costs avoided from not duplicating dispensing and using patients on medication on discharge was £201.38, a potential annual total of £2,600.
Discussion
The re-engineering achieved the prime aim of early, rapid but safe discharge. This in turn created the space for the pharmacist to have time to concentrate on more demanding clinical needs of head and neck cancer patients. The cost avoidance of over £2500 per year is probably an under estimate as the use of PODs and one stop dispensing has increased. Although not evaluated objectively the new system has elicited a lot of positive feedback from nursing staff on the ward. A number of other wards, particularly gynaecology and orthopaedics have expressed interest in a similar system. Complaints about delayed discharge have almost disappeared. Unfortunately it was not possible to evaluate accurately changes in TTO processing time, as the new model does not record the time of TTO being written and finished. This is unlike the traditional dispensary based service, where arrival and departure of TTOs is logged. However the fact that almost all TTOs dispensed on the ward are in patients' hands by 10.00 am, and frequently earlier, represents a considerable improvement in service. There is considerable added value as most patients also get medication counselling from the pharmacist.
There were concerns that a model, which concentrated activity on the provision of discharge medication may have become product centred and detracted from the clinical role of the pharmacist. The fact that the intervention rate was about 2 interventions per day indicates that this is not the case. The number of interventions made by the pharmacist was greater but only the interventions for ENT patients were recorded. Over the study period there were significant numbers of medical and other surgical patients in the ward and interventions for them were discounted.
Conclusions
Re-engineering pharmaceutical care in ENT to concentrate on patients needs can provide a positive outcome for patients as well as improve the value for money of services.